
Name: Monica (child), Lyn (mother)
Child: 3 years old
City and state: St. Louis, MO
Areas of involvement: bilateral, upper extremities
Personal History:
I am the mother of a 3-year old girl, Monica, who was diagnosed with melorheostosis approximately a year-and-a-half ago. Monica is our seventh child. We are "older" parents (I will be 47 in March), and with the exception of one child who died in utero, our six other children have been pretty healthy.
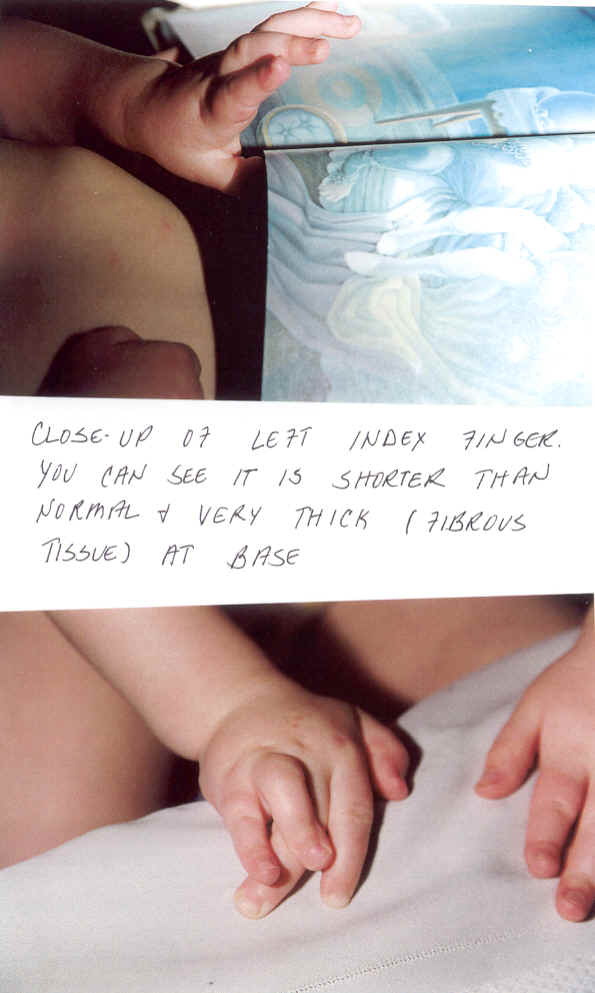
When Monica was 4 days old, we noticed that one of her fingers on her right hand was contracted and twisted. Because newborns tend to keep their fists clenched, neither I nor anyone at the hospital had noticed. I took Monica to her pediatrician who thought that perhaps she had broken her finger during vaginal delivery. We had x-rays done, but they showed nothing abnormal. (In looking back, the x-rays at this early age would probably not have been helpful since they do not show much calcification or the bony structure one sees in later maturity.) But something was definitely not right. Over the next few months, other fingers began to show characteristics of problems. Her (right "ring"-- fourth) finger that was contracted got much worse and grew sideways over the finger next to it. Her index finger on her left hand did not grow in proportion to her other fingers and became hyperextended (bent backwards) and rigid. It also was very thick around its base. Her entire arm seemed sluggish,and her right side was obviously weak. Her chest became concave. Needless to say, we were scared to death. We took her to an orthopod at approximately 6 months of age who x-rayed her hands and arms and could find nothing amiss. Hoever, he did find severe dysplasia of the hips and said she might have to undergo corrective surgery for this if the problem did not self-correct. (Later x-rays done at approximately 17 months of age showed no evidence of this problem so the problem obviously self-corrected.) We also took her to a nuerologist due to the obvious weakness in her right side (by six months, she could not roll over). He found nothing in the way of a diagnosable neurological condition, but ordered occupational therapy to strengthen her right side.
The occupational therapist helped Monica develop her strength and educated me on hand and arm deformities/problems. She was very concerned about Monica, and said she had nevery seen such an array of different hand deformities: deviated wrists, hyperextended fingers, boutinere deformities, swan-neck deformities (the latter two are when the fingers either curve in or out at the mid or top knuckle), a lazy thumb on the left hand, a shortened finger on the left hand: a virtual garden of deformities! Armed with the information that the occupational therapist had given me, we took Monica back to the pediatrician and told him that we had to get to the bottom of what was causing her deformities. He sent me back to the orthopod who took another x-ray of Monica's hands and arms (by now, she was about a 14 months old). This time, the x-rays revealed calcium streaks and the hyperostosis (thick bone growth) that characterizes melorheostosis. However, the orthopod had no idea what was causing this because he had never seen an x-ray quite like it. When six weeks had gone by, and we still had no word from this doctor, we took Monica back to the pediatrician and demanded that we see someone who could tell us what we were dealing with. He referred us to Children's Hospital in St. Louis (which is where we live). A radiologist who is quite well known on a national basis--Dr. Bill McCallister-- made the diagnosis immediately after reviewing the films. However, since melorheostosis is so rare, and since it had never been diagnosed locally in anyone as young as Monica, he had three other radiologists look at the film and give their own independent diagnoses. The unanimous consensus/diagnosis was bilateral melorheostosis of the upper extremities. The skeletal survey done on Monica revealed melorheostosis in the left scapula, the left proximal humeral epiphysis, the left distal humerus, the left proximal ulna, the right distal humerus and right proximal ulna. (Medical terms for various bones in the shoulders, arms, and wrists.) In addition, the right and left hands were extensively affected, with the most severe involvement in the second, third, fourth and fifth fingers of her left hand and the third and fourth of her right hand. There is associated soft tissue deformity, with the fourth finger crossing over the third on the right hand and the second finger on her left hand rigid, and basically unable to move.
Subsequently, we were referred to Shriner Hospital in St. Louis where the hand surgeon suggested osteotomies on the third and fourth fingers of Monica's right hand. We did not fully accept the surgeon's recommendation because we felt that he and his staff were unreceptive to our questions and input. Specifically, I was concerned about research showing that surgery on children with melorheostosis has a history of poor outcomes. I was particularly concerned about the need for a repeat of surgery due to the high recurrence of soft tissue deformity. We decided to seek a second opinion.
This past June, my husband and I went to Mayo's Clinic in Rochester, Minn. We saw two doctors there: Dr. Anthony Stans, an orthopod who has seen or is seeking 5 other children with melorheostosis, and Dr. Julia Katarincic, a hand surgeon. Their opinion was that Monica did need surgery within the year on both hands: osteotomies on two of her fingers on the right hand and an osteotomy on her left index finger. They also recommended an MRI of Monica's left hand because she has a palpable mass (thickness) in the palm below her left index finger which is the same one that is rigid and paralyzed. They also told us that they are sure that the surgery will need to be repeated since soft tissue deformity recurrence is part of the disease, especially in children. Therefore, they said it would be okay for us to wait about one more year before having the surgery done since Monica will undoubtedly have to undergo it a second time.
Unfortunately, our insurance would not allow us to have the surgery at Mayo's. We went ahead and had an MRI done on both of Monica's hands in September of this past year. The "mass" in Monica's hand is not a tumor, but simply a thick overgrowth of tissue. (The doctors had wanted to rule out the possibility of a desmoid tumor, even though such tumors are not likely to be found in the hand. Desmoid tumors are associated with melorheostosis, and although benign can apparently be aggressive.)
At this point, we have found a new hand surgeon in St. Louis, Dr. Mitch Rotman of Cardinal Glennon Children's Hospital, who is wonderful insofar as he is willing to listen to our input and do research with us on melorheostosis. In late spring or early summer, Monica will undergo her first surgery-- an osteotomy on her left index finger. We will take one hand at a time so that she can have the use of her other while recovering. Also, we thought that it made sense to start on one finger and see how it did following surgery, with the idea that perhaps this would give us a clue as to how Monica's bones will heal.
As is typical of melorheostosis in children, Monica is in no pain, although if you saw her crooked and twisted fingers, you would swear that she had to be. However, we are fully aware that pain, often beginning in the pre-adolescent years, is part of this disease. In sharing our experience, we are prayerful that others will be motivated to talk about theirs and possibly, we can someday interest researchers to pursue further study of this disease. We believe that the hope of a "cure" or "treatment" of this disease lies in finding its pathogenesis and the genetics that govern it. We also believe that, despite the fact that melorheostosis is classified as extremely rare, there are more people out there that have it than the literature would lead one to believe. The only way we can find out is by sharing our experiences with one another and spreading the word of this website. We are thrilled and very excited that the site is being launched and hope that it will attract the attention of melorheostosis sufferers, doctors and researchers.
UPDATE REGARDING SUBSEQUENT SURGERY (9/2001)
Monica had surgery on her left index finger. The purpose of the surgery was to restore mobility to her left index finger which has been virtually "frozen" in a hyper extended position since she was an infant. This surgery involved removing the "capsules" from her mid- and lowest (next to the hand) knuckles and then "scraping" the cartilage that extends between those two knuckles into a more contoured, rounded shape. The surgery entailed placing a couple of pins through her bones: one in the upper part of her finger and one in the lower part. The pins were exterior pins: in other words, they went all the way through the finger and extended to the outside. Then, rubber bands were placed between each set of pins to provide artificial flexion and to bend the finger downwards. In addition, a splint was placed over her hand which also exerted considerable downward pressure on her finger.
The surgery was fraught with complications. Twice during surgery when they tried to attach the rubber bands, Monica's circulation to the finger cut off. As soon as the rubber bands were removed, the circulation returned, leading the surgeons to conclude that Monica's circulation to the finger was less than optimal. A decision was made to postpone placement of the rubber bands until several days following surgery when some of the trauma of surgery had subsided. Five days after surgery, the rubber bands were placed on the pins. Within a day of that, Monica developed a very serious infection of the finger. She ended up in the hospital for 8 days on IV antibiotics. For a while, she did not appear to be responding to the antibiotics, and we were scared she might lose the finger altogether. However, she eventually did respond. But in the interim, the pins all had to be removed. The finger is now bright red (scar tissue), and it does not function significantly better than before surgery (and looks much worse).
As a result, her doctor has prescribed intense occupational therapy for Monica: 3 times a week at the hospital, and 5 times a day at home. This involves bending the finger up and down several times, and exerts considerable force on her mid- and lower knuckles. The doctor and therapist say that it is essential we do this because if Monica's finger heals with all the scar tissue, she will have no movement in it as before. There will have been no point to the surgery.
I cannot begin to describe the pain that the therapy causes Monica. She screams and cries, and has even wet her pants and thrown up while we are doing it. The therapist tells me that such pain is not uncommon, and that it is necessary if she is ever going to regain movement. Monica HAS moved her finger, but it is such small movement that it would be undetectable to most people.
I continue to do this therapy, but it is causing me great stress. I am totally depressed by how fearful Monica has become. If I knew the therapy was actually going to help, I would weather the situation and put up with Monica's pain. I realize that MANY parents have to experience and cope with their child's pain when they undergo painful, but necessary, medical procedures. But is this necessary? Is it going to help?
Here are my questions:
1) Has anyone ever had successful surgery, especially on a finger, which was immobilized by melorheostosis?
2) Has occupational therapy ever proved helpful to anyone, especially post-surgically?
I would greatly appreciate ANY feedback from others on the website.
Thank you, Lyn (Monica's mother)
![]()